JOURNAL CLUB - Strategies for lung- and diaphragm-protective ventilation in acute hypoxemic respiratory failure: a physiological trial
By: Marcelo Alcantara, Médico - 09/02/2022 16:31
🤔Is it feasible to achieve physiological or safe spontaneous respiratory effort and distending pressures in intubated patients with moderate to severe acute hypoxemic respiratory failure (AHRF)?
👨⚕️Seventeen investigators (16 from Toronto, Canada, and one from São Paulo, Brazil) addressed this question in an interesting physiological trial. Their study was published on 29th august 2022 in Critical Care.
🧐They evaluated 30 patients with moderate to severe AHRF of various etiology, mainly COVID-19 and pneumonia, that were intubated and ready to transition from controlled to assisted ventilatory support.
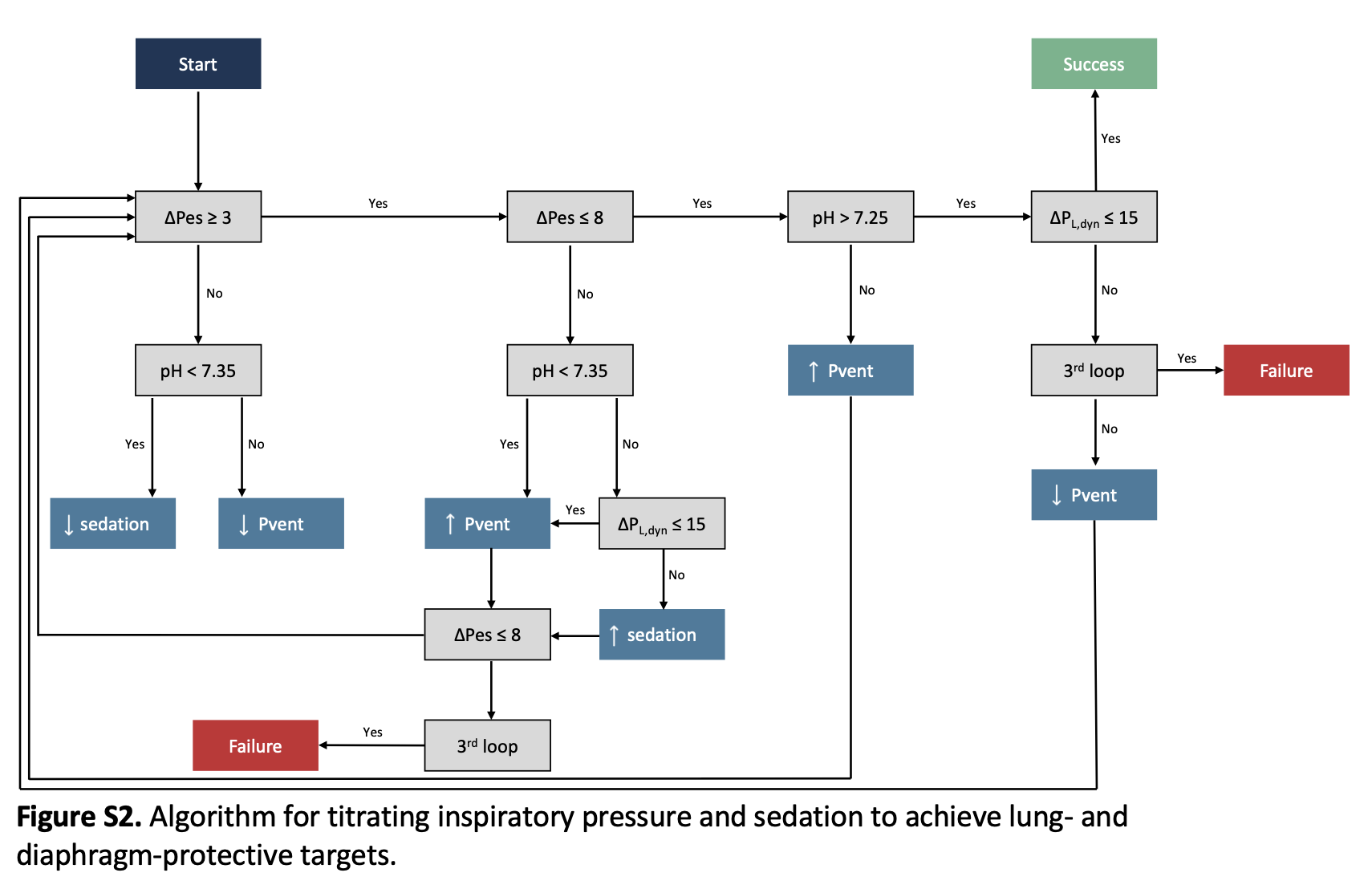
🧐The intervention adopted a pre-designed algorithm to maintain the following targets for the respiratory effort, esophageal pressure swings, ∆Pes, −3 to −8 cmH2O, and distending dynamic transpulmonary pressures ∆PL,dyn ≤ 15 cmH2O. They called this strategy Lung and Diaphragm Protective (LDP) ventilation.
Please see the algorithm in the figure below.
🧐An experienced physician and respiratory therapist constantly attended at the bedside throughout the protocol.
🧐A combination of interventions was set in the algorithm, including sedation depth and level of pressure delivered by the ventilator to achieve LDP targets. Additionally, partial neuromuscular blockade (pNMBA) with low doses of cisatracurium was administered in patients with refractory excessive respiratory effort. The sweep gas was titrated in patients with VV-ECMO to achieve the targets. Finally, the PEEP was tested in patients with either high or low levels to assess its effect on the amount of respiratory effort in a cross-over design.
👉The main result was that LDP targets were achieved in 20/30 patients. LDP targets were more likely to be achieved in patients on VV-ECMO (median OR 10, 95% CrI 2, 81). Administration of pNMBA to patients with excessive refractory effort was well-tolerated and effectively achieved LDP targets. The main physiological variables are shown in the figure below.

🧐The authors conclude that achieving somewhat safe levels of both respiratory effort and distending pressures in intubated patients with AHRF after an initial period of controlled mechanical ventilation is possible. The effect of PEEP was not predictable. It attenuated respiratory effort only when higher levels resulted in better respiratory compliance.
💪Strengths of the study.
The rationale and the intervention to investigate the central hypothesis were very well matched. The study answered its main question.
😒Limitations. Absence of blindness, a stringent and complex protocol to apply at the bedside (it probably needs a high level of expertise in the field), and a short-term investigation period.
🤔Does it change my practice at the bedside? Well, it points out the optimization and individualization of PEEP, pressure support, or pressure above PEEP in PCV and sedation in AHRF during assisted ventilatory support. Furthermore, we must be cautious during sedation titration and withdrawal in these patients. In general, they "wake up" with excessive respiratory drive and effort increasing the risk of patient self-inflicted lung injury (P-SILI). Respiratory monitoring is another issue highlighted by the paper. The respiratory pattern, including the level of the respiratory drive, estimated Pmus, and dynamic driving pressure, must be considered to guide the level of both ventilatory support and sedation. The use of VV-ECMO was effective in achieving LDP targets. In particular, the titration of the CO2 washout by the sweep gas is of paramount importance.
Below is the link to the full-text paper.
Please take a little time to send us your personal opinion about the paper and our comments. Did you like it? Please share with your colleagues, fellows, or students.
To add an answer on this topic and read the replies...
You must have a valid and active xlung subscription
If you are already a subscriber, please Login at the top of the page, or subscribe now